POLYPS AND SIGNIFICANCE IN FERTILITY
Endometrial polyps are focal growths of the uterine mucosa and consist of endometrial glands, stroma and blood vessels. Uterine polyps are found in 10 % of female population .They are mostly identified during investigations for abnormal uterine bleeding and infertility.
Association between endometrial polyps and subfertility is controversial, many women with polyps may have successful pregnancies. Recently studies have shown that the polyps are related to fertility.
Prevalence of Endometrial Polyps in Infertile Women
Prevalence of such unsuspected polyps, diagnosed by hysteroscopy prior to in vitro fertilisation (IVF), has been described to be between 11 and 45 % . Endometrial polyps also appear to be the most commonly detected abnormality (16.7 %) in patients with recurrent implantation failures after IVF . It is suggested that polyps have higher incidence in women with endometriosis(46.7 %).
Mechanisms of Polyp–Subfertility Association
It is related to mechanical interference with sperm transport, embryo implantation or through intrauterine inflammation or increased production of inhibitory factors such as glycodelin.
Pregnancy rate within 6 months after polypectomy is 57.4 % for polyps located at the uterotubal junction, 40.3 % for multiple polyps, 28.5 % for posterior wall polyps, 18.8 % for lateral wall polyps and 14.8 % for anterior uterine wall polyps . There was no difference in pregnancy or miscarriage rates between women who had polypectomy for a small (≤1 cm) and those who had surgery for a bigger or multiple polyps . Lack of association between the size of polyps and fertility goes against a mechanical effect.
Glycodelin, a glycoprotein, inhibits sperm-oocyte binding and NK cell activity. In ovulatory endometrium, glycodelin levels are very low between 6 days before and 5 days after ovulation. Low glycodelin levels facilitates fertilisation, the levels increase significantly 6 days after ovulation to suppress NK cell activity and render the endometrium receptive to implantation. It is speculated that fertilisation and endometrial receptivity may be altered by increased glycodelin production in the uterine cavity of patients with leiomyomas and polyps in the periovulatory period.It is seen that the presence of polyps may alter HOXA10 and HOXA11 gene expression, molecular markers of endometrial receptivity, and impair endometrial receptivity in uterus with polyps .
Diagnosis
To evaluate endometrial polyps commonly a two- or three-dimensional transvaginal ultrasound is used.The diagnostic accuracy of 2D TVUS is poor compared with other diagnostic modalities such as saline infusion sonography (SIS) or hysteroscopy. Endometrial polyp is suspected by the presence of a hyperechogenic endometrial mass .
Performing the ultrasound examination in early proliferative phase, when the endometrium is thin, makes it easier to see the polyp. Sessile polyps can be confused by submucous fibroids. It might also be difficult to distinguish between a true polyp and polypoid endometrium by ultrasound.
Meta-analysis suggested that saline infusion sonography has a high degree of diagnostic accuracy in the detection of all types of intrauterine abnormalities with a sensitivity and specificity of 88 and 94 %, respectively. Hysteroscopy remains the gold standard in the diagnosis of endometrial polyps . Hysteroscopy also allows simultaneous treatment in the form of removal of the endometrial lesions.
If TVUS is suggestive of endometrial polyps,hysteroscopy is done. If the TVUS is inconclusive in an infertile and otherwise asymptomatic woman, 3D saline infusion sonography (3D SIS) is done.
Management
Some endometrial polyps may resolve spontaneously, regression has been observed in 27 % cases .
Endometrial polyps are removed as part of a hysteroscopic procedure, removal may be either a blind procedure using a curette or polyp forceps after hysteroscopic diagnosis, or under direct vision using operative minihysteroscopes or resectoscopes.It is seen that 10 % of intrauterine lesions, are missed during ‘blind’ curettage .Hysteroscopy directed polypectomy using scissors, loop electrode, electric probe or a morcellator is done to minimize damage to the surrounding endometrium and to ensure the polyp has been removed completely. The resectoscope is the method of choice , with least recurrence rate compared to electric probe, microscissors and grasping forceps .
Management and IVF
When suspected by ultrasound prior to stimulation for IVF or frozen embryo transfer (FET), polyps are further investigated and treated. Treatment options include continuation of ovarian stimulation followed by fresh transfer, freezing all embryos and replacement of frozen–thawed embryos after removal of the polyp, or cancellation of the treatment cycle and removal of the polyp. The factors that affect decision-making include the number of embryos created, previous reproductive history and the success rate of the FET programme, as well as the clinicians’ preference.
Studies suggest that patients with an endometrial polyp detected and resected before ICSI cycle had similar pregnancy rates compared with patients with no endometrial polyps. It is also seen that in case of polyps diagnosed during stimulation and <1.4 cm in size, it is not necessary to cancel the embryo transfer . Usually 3D SIS is routinely done before IVF cycles with fresh or frozen embryo transfer. In general, hysteroscopic polypectomy is done for polyps diagnosed before stimulation. If we diagnose a polyp during stimulation we counsel our patients and discuss different options of treatment based on available evidence. Freeze all embryos after egg collection and plan for a hysteroscopic polypectomy followed by a frozen embryo transfer cycle.
Cervical polyps
A cervical polyp is a small growth which occurs at the opening of the cervix, which may protrude into the vagina. These polyps are like a skin tag, often shaped like a fleshy bulb on a thin stalk .These growths are almost always benign and are usually quite tiny, rarely larger than 1 or 2cm. While cervical polyps are not dangerous, they can cause trouble, especially for women who are trying to conceive. There are two types of cervical polyps:
Ectocervical. Ectocervical polyps grow on the outer surface of the cervix. This type of polyp is usually seen in women who have gone through menopause. Ectocervical polyps are usually wider and shorter in shape.
Endocervical. Endocervical polyps grow from glands inside the cervical canal, and tend to occur in women of childbearing age. These polyps generally have a longer stalk.
CAUSES:-
Cause is not fully understood, they are often associated with hormone changes in the body. Issues with body’s response to estrogen, which may cause an over-stimulated growth of cervical tissue.Women with polyps also had polycystic ovarian syndrome (PCOS). Body mass index of women with polyps was significantly higher than women without polyps. Women with more body fat produce higher levels of estrogen.
Chronic inflammation. We do know that women with diabetes (an autoimmune disorder) and recurrent vaginitis infections are more prone to polyps.
Symptoms of cervical polyps and diagnosis
Most cervical polyps are asymptomatic.
Irregular or heavy periods.
Spotting between periods or after sexual intercourse.
A foul-smelling discharge.
For some women, infertility is the only symptom of cervical polyps.
Cervical polyps and fertility
Polyps high up in the cervix can block the opening of the cervix and make it impossible for fertilization to occur. In some cases, it may interfere with the production of cervical mucus.
Treatment
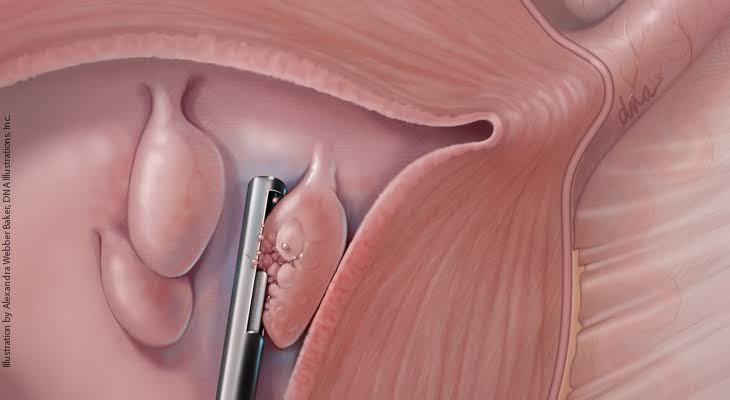
Using a special pair of small forceps called polyp forceps the polyp is grasped at its base, and then gently twist and tug to remove the growth.
Conclusion
Endometrial polyps are commonly seen in subfertile women. Use of appropriate and sensitive diagnostic tests for subfertility and prior to fertility treatment is commonly performed with good detection rates. Data available on removal of polyps and spontaneous pregnancy or intrauterine insemination success rates suggest a potential benefit.